The NHS capacity crisis hiding in plain sight. Why small changes deliver the gains that big programmes never do.
Comments Off on The NHS capacity crisis hiding in plain sight. Why small changes deliver the gains that big programmes never do.Every NHS trust has a capacity problem. Almost none of them have accurately measured where that capacity is actually going. Those are connected facts, and the connection between them is where most improvement programmes quietly fail.
The wrong unit of change
When an NHS service faces a capacity crisis, the response follows a familiar pattern. A review is commissioned. Options are assessed. The conclusion almost always involves more: more sessions, more staff, more space, more budget. The scale of the problem is matched, in theory, to the scale of the solution.
This instinct is understandable. It is also, in most cases, wrong.
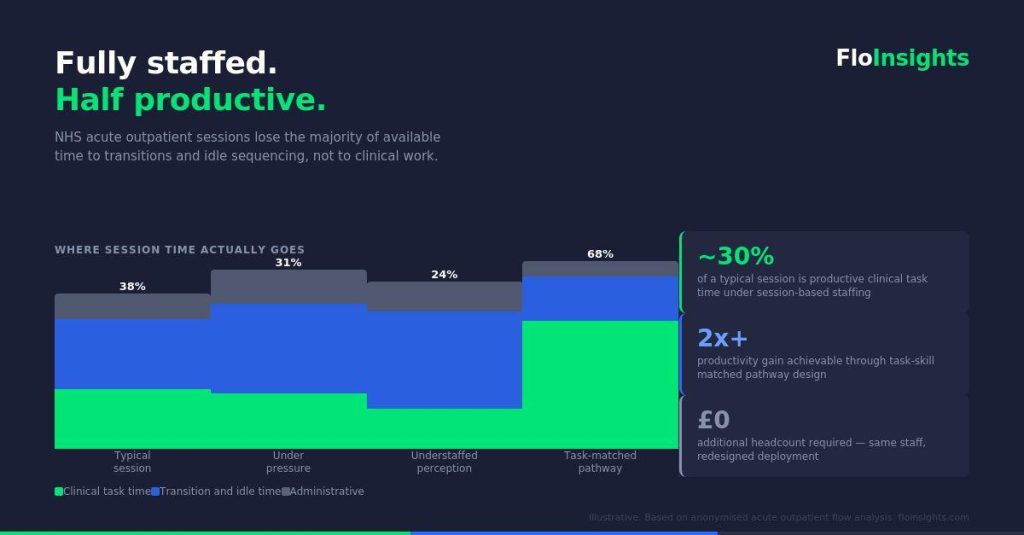
The problem with large-scale capacity interventions is not that they never work. It is that they consistently overestimate what resource can achieve when the underlying constraint has not been precisely identified. You can add a session to a service that is losing capacity through poor flow sequencing and find that the new session loses capacity at exactly the same rate. The resource has changed. The constraint hasn’t.
The more productive question is not how much resource to add. It is where, precisely, is the capacity being lost, and what is the smallest targeted change that moves that specific constraint. That question requires data. It requires measurement at a level of granularity that most NHS services do not currently apply to their own operations. And it requires a methodology that prioritises speed of action over scale of intervention.
What marginal gains actually means in an operational context
The aggregation of marginal gains is a concept most people associate with elite sport. James Clear’s Atomic Habits brought it to a general audience: the idea that a one percent improvement in each of many small areas compounds over time into results that dwarf what any single large change could achieve.
Clive Woodward’s transformation of England rugby is the example that belongs in this conversation. Woodward did not inherit a squad of world-class players and win the World Cup. He identified every single variable that affected performance, many of them things previous coaches had not thought to measure, and improved each one incrementally. The analytical rigour he applied to marginal factors, nutrition, sleep, video analysis, legal strategy, was as important as any tactical decision on the pitch. England won in 2003 because of a system, not a moment.
The parallel with NHS operational improvement is exact. Services that improve sustainably do so not because they find one transformational change but because they build a system for identifying, prioritising, and compounding small improvements continuously. The methodology is the advantage.
What is missing from most NHS improvement programmes is precisely that: the systematic identification of where the marginal gains are, the prioritisation of which ones to take first, and the measurement infrastructure to know whether each change has worked before moving to the next.
Two case studies in small changes with large consequences
The following observations are drawn from anonymised analysis of high-volume acute outpatient services. No patient-identifiable data is used or referenced.
Case one: one hour removed from every patient’s wait in twelve weeks
A high-volume acute outpatient service was experiencing waiting times that its team attributed to insufficient staffing. The instinct was to request additional resource.
Before any resource decision was made, pathway flow data was analysed across the four quotients of the FloInsights Benchmarked Operating System: Workforce, Patient Flow, Space and Equipment, and Finance. The analysis identified that the constraint was not total staffing level but load distribution. Resource was not evenly matched to demand across the session. At specific points in the pathway, a bottleneck was forming that downstream capacity could not recover from.
The intervention was precise: accurate load balancing and targeted redeployment of existing resource to the point of constraint. No new staff. No new budget. No reorganisation.
Within twelve weeks, patient waiting time had reduced by one hour per patient across the service. The capacity had always been there. The data made it visible and the prioritisation made it actionable.
Case two: 33% more capacity from one flow change

A second service was operating at a level that clinical and operational leads considered close to maximum capacity. The consultant, the highest-cost and most clinically scarce resource in the pathway, was involved at multiple points across the patient journey, many of which did not require consultant-level skill.
The analytical question was simple: what in this pathway can only the consultant do? The answer, when mapped against actual task data, was narrower than anyone had assumed. A significant proportion of consultant time was being consumed by tasks that, with appropriate support and redesign of the surrounding pathway, could be safely and effectively handled at a different skill level.
The initial change was small. A single adjustment to the flow sequence, redistributing one category of task away from the consultant and building support around the remainder of the patient journey.
The result was a 33% improvement in capacity with identical resource. The consultant was freed to work at the top of their clinical capability. The pathway was faster. Patients moved through more efficiently. The service could absorb more volume without adding cost.
One flow change. A third more capacity.
Why this keeps not happening
If small, targeted, data-identified changes consistently outperform large resource interventions, the question is why NHS services don’t pursue them systematically.
The answer has several components.
The data is not in usable form. Session-level activity data is abundant. Pathway-level flow data, the kind that shows precisely where time accumulates, where constraints form, and where the highest-value intervention points are, is rare. Most services cannot see their own operations at the level of granularity required to identify marginal gains. They know roughly what happens in a session. They do not know exactly where each minute goes.
The prioritisation framework doesn’t exist. Even where data is available, the question of which change to make first is not systematically answered. Improvement programmes tend to be driven by clinical opinion, management instinct, or political priority rather than by a structured analysis of which intervention delivers the greatest gain for the smallest disruption. The result is that available improvement energy is not always directed at the highest-value opportunities.
The measurement cycle is too slow and requires too many hours, too much effort. It is episodic. NHS improvement programmes typically evaluate impact over months or years. By the time data confirms whether an intervention has worked, the operational context has changed, staff have moved on, and the learning is lost. A monthly measurement cycle, tied directly to the specific change that was made, is what allows gains to compound rather than dissipate.
The Benchmarked Operating System
The FloInsights BOS, Benchmarked Operating System, is built around the insight that the methodology is the advantage.
Analysis is structured across four quotients: Workforce, Patient Flow, Space and Equipment, and Finance. Each quotient surfaces a different dimension of where capacity is being generated or lost. Together they provide a complete operational picture that session-level data alone cannot deliver.
From that benchmarked baseline, rapid, data-driven and prioritised action plans are generated. Not large transformation programmes. Specific, small, high-value interventions identified by the data and sequenced by impact. The smallest change with the greatest consequence goes first.
Monthly measurement closes the loop. Each change is tracked against the baseline. Gains are confirmed and compounded. The next priority is identified. The cycle repeats.
This is not a consultancy model that delivers a report and leaves. It is an operating system that builds the measurement infrastructure into the service itself, so that the capacity to identify and act on marginal gains becomes a permanent organisational capability rather than a one-off project outcome.
The compounding argument
Clive Woodward’s England did not improve by finding one thing that made them 33% better. They improved by finding thirty things that each made them one percent better, and building a system that kept finding the next one.
The same logic applies to NHS acute outpatient capacity. A service that reduces waiting time by one hour in twelve weeks through one precise intervention, and then finds the next constraint, and then the next, is not on a linear improvement curve. It is on a compounding one.
The capacity gains available to most NHS services through this approach are larger than any resource programme currently being contemplated. They do not require additional budget. They require accurate measurement, disciplined prioritisation, and a monthly cadence of action and review.
The data to start is already in the service. The question is whether it is being used.
These case studies are drawn from anonymised analysis of high-volume acute outpatient services. No patient-identifiable data is used or referenced. FloInsights works with NHS trusts and healthcare organisations to make pathway-level operational data visible and actionable through the Benchmarked Operating System.
To discuss how this applies to your service, contact us at insights@floinsights.com