
The staffing model NHS services inherited was built for a different era of medicine. It was built when clinical tasks were less differentiated, when skill mix meant doctor and nurse, and when the bottleneck in outpatient care was usually the consultant’s availability. That era has gone. The staffing model hasn’t.
The question nobody is asking
Every operational review of an NHS acute outpatient service eventually arrives at the same conversation. Waiting times are too long. Lists are too short. The solution proposed is almost always some version of more: more sessions, more staff, more resource.
It is a reasonable instinct. It is also, in most cases, the wrong diagnosis.
The question that rarely gets asked is not how many people are in the room. It is whether the right skills are deployed at the right points in the pathway, in the right sequence, at the right time. Those are different questions. They have different answers. And the gap between them is where NHS outpatient productivity quietly disappears, in ways that never appear on a job plan or a rota.
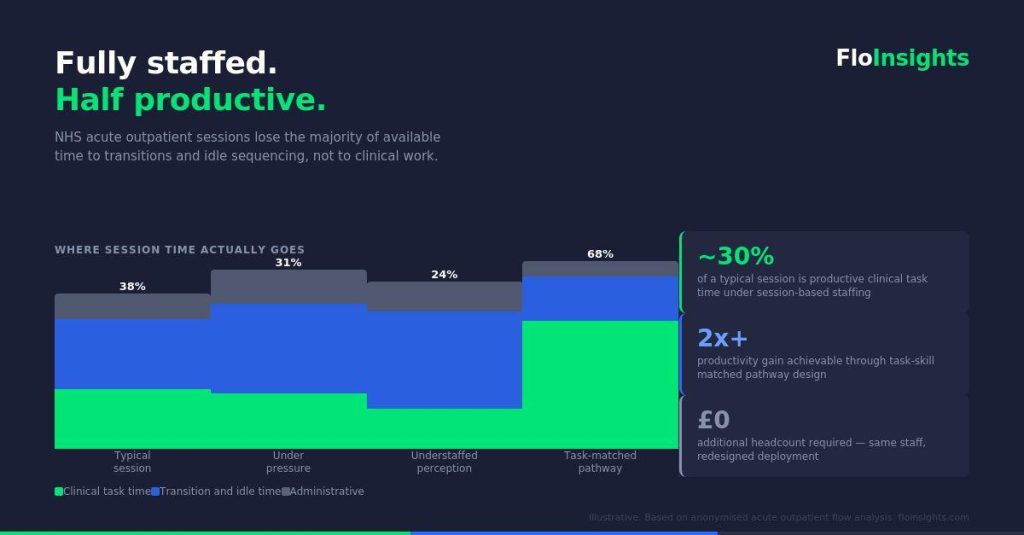
This piece makes a simple argument: the NHS staffing model for acute outpatient services is built around session coverage rather than task-skill matching, and that mismatch is a structural productivity ceiling that more headcount cannot solve.
How NHS outpatient services are actually staffed
The unit of workforce planning in NHS outpatient services is the session. A session is a time block, typically three to four hours, within which a defined set of staff are present and a defined number of patients are scheduled. Job plans are built in programmed activities, which are session-equivalent units. Rosters are constructed to ensure session coverage. Agency and bank staff are booked per session. Performance is measured as activity per session.
This model has an internal logic. Sessions are plannable. They are contractually legible. They map to the way NHS facilities are booked, the way consultants’ time is contracted, and the way activity data is reported upward.
The problem is that sessions are a time-based unit, and clinical productivity is not a time-based phenomenon. It is a sequence-based phenomenon. What determines how much valuable clinical work gets done in a given period is not how many staff are present for how long. It is whether the right skills are available at each decision point in the pathway, and whether the pathway is designed to make that matching possible.
When those two things are misaligned, you get a service that is fully staffed on paper and structurally constrained in practice.
What flow data shows
Analysis of patient flow in high-volume acute outpatient settings produces a consistent and instructive picture.
The clinical tasks within these services, the skilled assessments, the diagnostic procedures, the clinical interventions, tend to execute with high consistency. When a trained clinician performs a defined task within their competency, the duration of that task is relatively stable. It does not vary much with session pressure. It does not stretch significantly when the clinic is busy. Skilled clinical execution, in other words, is not where the variability lives.
The variability lives between the tasks.
When you track patients through a multi-step outpatient pathway, the time that accumulates in ways unrelated to clinical complexity is almost entirely found in transitions: the movement from one step to the next, the wait before a task begins, the moment when one clinical input has been completed and the pathway needs to advance but the next input is not ready to receive the patient.
In a well-sequenced pathway with appropriate skill deployment, these transitions are short. In a pathway staffed by session coverage rather than task-skill matching, they lengthen. Not because anyone is working slowly. Because the sequencing of skills along the pathway has not been designed. It has been assumed.
The practical consequence is significant. A service can have consistent clinical task durations, good individual performance, and competent staff throughout, and still run at well below its productive potential, purely because the architecture of skill deployment creates idle time between tasks that compounds across a session and across a list.
The cost that never appears on a budget
NHS workforce costs are almost universally reported as a cost per session or a cost per whole time equivalent. Neither metric surfaces the question of whether high-cost skills are being used on high-complexity tasks.
Consider a typical acute outpatient pathway with three or four sequential clinical steps, each requiring a different skill level. If the staffing model has been built around session coverage rather than task-skill matching, it is common to find that senior clinical time is being consumed by tasks that sit below the threshold of that skill level, not because of negligence or poor practice, but because the session model does not distinguish between tasks. Everyone is booked for the session. The session runs. The activity is recorded.
What is not recorded is the cost of skill misallocation: the consultant time spent on tasks a specialist nurse could safely perform, the specialist nurse time absorbed by administrative steps, the healthcare assistant capacity that sits idle while upstream bottlenecks resolve.
This is not a minor inefficiency at the margin. In a high-volume service running multiple lists per week, the cumulative cost of skill misallocation, measured in productive clinical hours lost, can be substantial. It simply never appears as a line on a budget because the budget is not structured to make it visible.
The financial model and the operational model are using different units. Neither surfaces the problem. So the problem persists, and the solution proposed remains the same: more sessions.
Why job planning doesn’t solve this
The standard NHS response to outpatient productivity concerns is job planning review. Consultants’ programmed activities are examined. Ratios of direct clinical care to supporting professional activities are scrutinised. Session allocations are adjusted.
Job planning is a necessary process. It is not a sufficient one.
Job planning operates at the level of the individual clinician’s time allocation. It does not model the pathway. It does not map the sequence of tasks against the sequence of skills required. It does not ask whether the skill mix present in the session matches the task mix on the list.
A consultant can have a perfectly structured job plan and still spend a significant proportion of their direct clinical care time waiting for a pathway step that a different skill should have completed earlier, or completing a task that a different skill could complete safely and at lower cost. The job plan is clean. The deployment is inefficient. The job plan review finds nothing to change.
Pathway-level skill deployment analysis is a different discipline. It requires modelling the patient journey as a sequence of discrete tasks, mapping the skill requirements of each task, and then asking whether the staffing model in place makes that sequence flow efficiently. It is an operational design question, not a workforce planning question in the traditional sense.
What good looks like
A service designed around task-skill matching rather than session coverage would look different in several specific ways.
Skill mix would be determined by pathway task analysis rather than professional convention. The question “who needs to be in this session?” would be answered by mapping what tasks need to happen, in what sequence, and what skill level each requires, rather than by replicating the staffing pattern of the previous year.
Sequencing would be explicit. The order in which patients move through pathway steps would be designed to minimise transition time and maximise the utilisation of scarce high-skill resource. High-cost skills would be protected from low-complexity tasks by appropriate delegation and task allocation upstream.
Productivity measurement would operate at the task level, not just the session level. The question would not be “how many patients were seen in this session?” but “how much of each skill type was deployed on tasks matched to that skill level, and what was the flow time between tasks?”
This is not a radical reimagining of clinical services. It is operational design applied to a sector that has largely been exempt from it. Manufacturing, logistics, and professional services have been doing task-skill matching for decades. The NHS, for understandable reasons rooted in professional structure and contractual history, has not.
The gap between those two positions represents a significant and largely untapped productivity reserve.
The data moat problem
There is a reason this argument has not been made more forcefully or more frequently. It requires data that most NHS services do not have in usable form.
Session-level activity data is abundant. Pathway-level flow data, the kind that shows task durations, transition times, and skill deployment sequences at the individual patient level, is rare. Most trusts cannot tell you how long each step in an outpatient pathway actually takes, how that varies by patient complexity or time of session, or where in the sequence idle time accumulates.
Without that data, the argument remains theoretical. With it, it becomes actionable. You can show precisely where the deployment mismatch occurs, quantify the productive hours lost, and model the impact of redesigning the skill sequence.
This is not a technology problem. The data exists in most services, in appointment systems, in clinic management software, in observation and audit records. It is an analytical problem: extracting, cleaning, and structuring that data in a way that makes the pathway visible as a sequence rather than as an aggregate.
When services can see their pathways in that level of detail, the conversation changes. The question stops being “how many staff do we need?” and starts being “how do we deploy the skills we have so that each one is working at the top of its capability, in the right place, at the right time?”
That is a more productive question. It tends to have a more productive answer.
The implication for workforce strategy
None of this is an argument against adequate staffing. Services need sufficient resource. The case being made here is narrower and more specific: that session-based staffing models create a structural ceiling on the productivity of whatever resource is deployed, and that ceiling cannot be raised by adding more of the same resource.
The implication for workforce strategy is that skill mix design needs to become a first-order question in outpatient service planning, not an afterthought to headcount decisions. Pathway task analysis needs to precede staffing model design, not follow from it. And productivity measurement needs to develop the granularity to surface skill misallocation, not just aggregate activity.
For finance directors and operational leads, this reframes the efficiency conversation. The question is not only what a session costs, but what productive clinical value that session generates per skilled hour deployed. Those are different numbers. In most services, the gap between them is larger than anyone has formally measured.
Closing that gap does not require more resource. It requires better information about how the existing resource is actually being used, and the analytical capability to turn that information into operational decisions.
That is a solvable problem.
These observations are drawn from anonymised analysis of patient flow data across acute outpatient settings. No patient-identifiable data is used or referenced. FloInsights works with NHS trusts to make pathway-level operational data visible and actionable.
To discuss how this analysis applies to your service, contact us at insights@floinsights.com